The EsophyX® Device: making transoral reconstructive surgery possible
Designed to reconstruct the gastroesophageal flap valve (GEFV) and restore its function as a reflux barrier, the EsophyX Device is used during the TIF® procedure to create a 3 cm, 270° esophagogastric fundoplication.
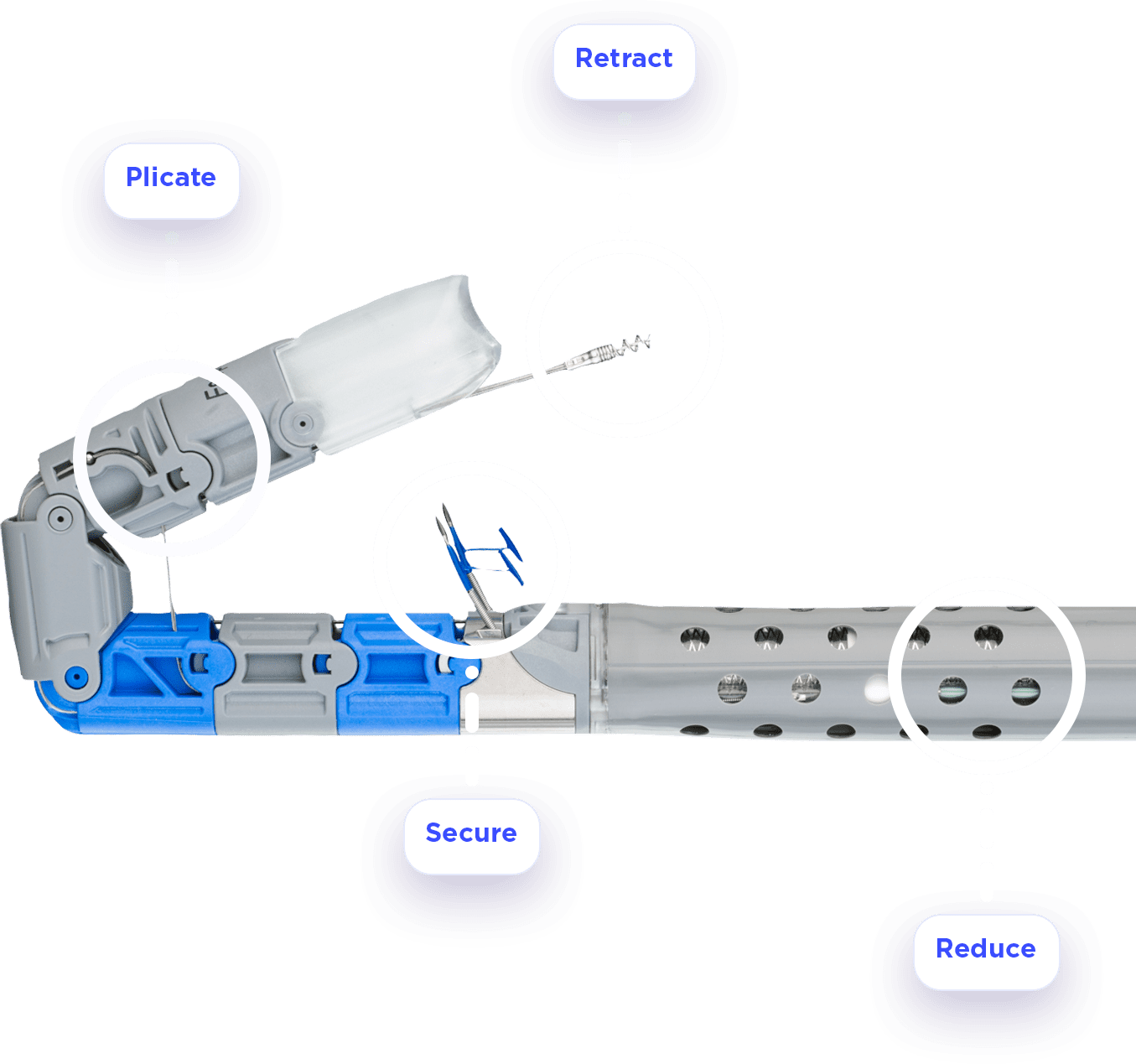
The EsophyX device utilizes proprietary tissue manipulating technology to deploy 20+ SerosaFuse fasteners that evenly distribute force across the entire circumference of the wrap – and all accomplished under direct endoscopic visualization with a flexible endoscope in the central lumen of the device.
The omega-shaped gastroesophageal flap valve (GEFV) built with the EsophyX device restores patient anatomy to its natural state and creates a reproducible and standardizable fundoplication without variability by utilizing endoscopic visualization, which contributes to the exemplary safety profile and minimal side effects…even in patients with hiatal hernias.
Strength you can trust: SerosaFuse® Fasteners
SerosaFuse fasteners are made of non-resorbable polypropylene and have equivalent web strength to a 3-0 suture. The material is durable, non-absorbable, and biocompatible, minimizing local inflammation and allowing natural GI tissue repair.
The SerosaFuse fasteners are deployed by the EsophyX devices to facilitate esophagogastric tissue plications and help evenly distribute force across the entire circumference of the wrap.
Effective reflux relief without the side-effects




“In my clinical experience, greater than 80% of my patients can come completely off their PPI’s.”